E-7
High Performance Single Use Pulse Lavage

Flexibility for efficient joint arthroplasty and trauma surgery
With its ease of use and effective cleaning, the Single Use Pulse Lavage offers efficiency and convenience throughout the application, resulting in potential reduced risk of revisions for the patient.
Pulsative lavage systems are being used with increasing frequency for total joint replacement. Several studies show that with high pressure pulse lavage, the cement penetration is increased. One of the main purposes for using high pressure pulsative lavage systems is to remove blood and debris during joint arthroplasty.
The Single Use Pulse Lavage system is used to clean the bone bed and soft tissue during the joint arthroplasty and trauma surgery.
With its ease of use and effective cleaning, the Single Use Pulse Lavage offers efficiency and convenience throughout the application, resulting in potential reduced risk of revisions for the patient.
Pulsative lavage systems are being used with increasing frequency for total joint replacement. Several studies show that with high pressure pulse lavage, the cement penetration is increased. One of the main purposes for using high pressure pulsative lavage systems is to remove blood and debris during joint arthroplasty.
The Single Use Pulse Lavage system is used to clean the bone bed and soft tissue during the joint arthroplasty and trauma surgery.

Improved clinical outcome with high pressure pulse lavage

Clean Bone Bed – Improved
bone cement interface
Effective bone bed preparation is one of the corner stones in Modern Cementing Technique. According to the Swedish Hip Arthroplasty Register the use of Modern Cementing Technique can lead to a signifi- cant reduction in the risk of revision.
Effective bone bed preparation is one of the corner stones in Modern Cementing Technique. According to the Swedish Hip Arthroplasty Register the use of Modern Cementing Technique can lead to a signifi- cant reduction in the risk of revision.
Effective cleaning for
optimal micro-interlock
A clean bone cavity, achieved with high pressure pulse lavage, ensures better cement penetration than with syringe lavage.This improves the quality of the bone cement interface, reduces the risk of blood lamination and enhances the mechanical strength of the cement.
A clean bone cavity, achieved with high pressure pulse lavage, ensures better cement penetration than with syringe lavage.This improves the quality of the bone cement interface, reduces the risk of blood lamination and enhances the mechanical strength of the cement.
High pressure pulse lavage
High pressure pulse lavage is a vital step towards achieving proper cement penetration and fixation into the cancellous bone.
High pressure pulse lavage has proven to be advantageous in removing debris and bone arrow from bone bed compared to syringes. It improves cement penetration and may also reduce the risk of embolic complications in joint replacement. Clinical studies have shown that the use of high pressure pulse lavage in total joint replacements may reduce the risk of revisions caused by aseptic loosening.
High pressure pulse lavage is a vital step towards achieving proper cement penetration and fixation into the cancellous bone.
High pressure pulse lavage has proven to be advantageous in removing debris and bone arrow from bone bed compared to syringes. It improves cement penetration and may also reduce the risk of embolic complications in joint replacement. Clinical studies have shown that the use of high pressure pulse lavage in total joint replacements may reduce the risk of revisions caused by aseptic loosening.
Reduced risk of fat embolism
High pressure pulse lavage used repeatedly during the cleaning sequence may prevent microembolisation of the marrow contents and significantly minimizes circulatory changes. The result of removing medullary content has been proven both experimentally and clinically to reduce risk of fat embolism. Not only the volume, but also the pressure of pulse lavage, influences the risk of fat embolism.
High pressure pulse lavage used repeatedly during the cleaning sequence may prevent microembolisation of the marrow contents and significantly minimizes circulatory changes. The result of removing medullary content has been proven both experimentally and clinically to reduce risk of fat embolism. Not only the volume, but also the pressure of pulse lavage, influences the risk of fat embolism.
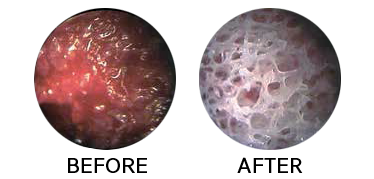

Images show before and after use of high pressure pulse lavage.
References
1. Malchau H, Herberts P, Garellick G, Söderman P,
Eisler T, (2002) The Prognosis of Total Hip Replacement,
Scientific exhibition presented at the 69th
Annual Meeting of the American Academy of Orthopaedic
Surgeons, February 13-17, 2002, Dallas, USA.
2. Lt. Scott Helmers, Peter F. Sharkey and LCDR Francis X. McGuigan. Efficacy of Irrigation for Removal of Particulate Debris after Cemented Total Knee Arthroplasty. Journal of Arthroplasty Vol. 14 No. 5 1999
3. Breusch SJ, Norman TL, Schneider U, Reitzel T, Blaha JD, Lukoschek M. Lavage technique in total hip arthroplasty: jet lavage produces better cement penetration than syringe lavage in the proximal femur. J Arthroplasty. 2000 Oct; 15(7):921-7.
4. Kalteis T, Pförringer D, Herold T, Handel M, Renkawitz T, Plitz W. An experimental comparison of different devices for pulsatile high-pressure lavage and their relevance to cement intrusion into cancellous bone. Arch Orthop Trauma Surg. 2007 Dec; 127(10):873-7. Epub 2007 Sep 1.
5. J.B. Seeger, MD, S. Jaeger, MSc, R.G. Bitsch, MD, PhD, G. Mohr, MD, E. Röhner, MD, and M. Clarius, MD, PhD. The Effect of Bone Lavage on Femoral Cement Penetration and Interface Temperature During Oxford Unicompartmental Knee Arthroplasty with Cement. JBJS Am. 2013 Jan 2;95(1):48-53.
6. Schlegel UJ, Siewe J, Delank KS, Eysel P, Püschel K, Morlock MM, de Uhlenbrock AG. Pulsed lavage improves fixation strength of cemented tibial components. Int Orthop. 2011 Aug;35(8):1165-9. doi: 10.1007/s00264-010-1137-y. Epub 2010 Oct 16.
7. Suvi Haimi, Marko Wahlman, Mari Mannila, Vesa Virtanen, and Martti Hirn. Pulse-lavage washing is an effective method for defatting of morselized allograft bone in the operating theater. Acta Orthopaedica, 2008; 79 (1): 94–97
8. Malchau H, Herberts P: Prognosis of total hip replacement in Sweden: Revision and re-revision rate in THR. Presented at the 65th Annual Meeting of the American Academy of Orthopedic Surgeons, New Orleans, LA, February 1998.
9. Breusch S J, Cementing Technique in Total Hip Replacement: Factors Influencing Survival of Femoral Components, Bone Cements and Cementing Technique, Springer Verlag, Chapter 4, Berlin Heidelberg 2001
10. J. Christie, C.M. Robinson, B. Singer, D.C. Ray. Medullary lavage during cemented hemiarthroplasty, J Bone Joint Surg [Br] 1995;77- B:456-9
11. Breusch S, Heisel C, Muller J, Borchers T, Mau H. Influence of cement viscosity on cement interdigitation an venous fat content under in vivo conditions: a bilateral study of 13 sheep. Acta Orthop Scand 2002 Aug; 73(4):409-15
2. Lt. Scott Helmers, Peter F. Sharkey and LCDR Francis X. McGuigan. Efficacy of Irrigation for Removal of Particulate Debris after Cemented Total Knee Arthroplasty. Journal of Arthroplasty Vol. 14 No. 5 1999
3. Breusch SJ, Norman TL, Schneider U, Reitzel T, Blaha JD, Lukoschek M. Lavage technique in total hip arthroplasty: jet lavage produces better cement penetration than syringe lavage in the proximal femur. J Arthroplasty. 2000 Oct; 15(7):921-7.
4. Kalteis T, Pförringer D, Herold T, Handel M, Renkawitz T, Plitz W. An experimental comparison of different devices for pulsatile high-pressure lavage and their relevance to cement intrusion into cancellous bone. Arch Orthop Trauma Surg. 2007 Dec; 127(10):873-7. Epub 2007 Sep 1.
5. J.B. Seeger, MD, S. Jaeger, MSc, R.G. Bitsch, MD, PhD, G. Mohr, MD, E. Röhner, MD, and M. Clarius, MD, PhD. The Effect of Bone Lavage on Femoral Cement Penetration and Interface Temperature During Oxford Unicompartmental Knee Arthroplasty with Cement. JBJS Am. 2013 Jan 2;95(1):48-53.
6. Schlegel UJ, Siewe J, Delank KS, Eysel P, Püschel K, Morlock MM, de Uhlenbrock AG. Pulsed lavage improves fixation strength of cemented tibial components. Int Orthop. 2011 Aug;35(8):1165-9. doi: 10.1007/s00264-010-1137-y. Epub 2010 Oct 16.
7. Suvi Haimi, Marko Wahlman, Mari Mannila, Vesa Virtanen, and Martti Hirn. Pulse-lavage washing is an effective method for defatting of morselized allograft bone in the operating theater. Acta Orthopaedica, 2008; 79 (1): 94–97
8. Malchau H, Herberts P: Prognosis of total hip replacement in Sweden: Revision and re-revision rate in THR. Presented at the 65th Annual Meeting of the American Academy of Orthopedic Surgeons, New Orleans, LA, February 1998.
9. Breusch S J, Cementing Technique in Total Hip Replacement: Factors Influencing Survival of Femoral Components, Bone Cements and Cementing Technique, Springer Verlag, Chapter 4, Berlin Heidelberg 2001
10. J. Christie, C.M. Robinson, B. Singer, D.C. Ray. Medullary lavage during cemented hemiarthroplasty, J Bone Joint Surg [Br] 1995;77- B:456-9
11. Breusch S, Heisel C, Muller J, Borchers T, Mau H. Influence of cement viscosity on cement interdigitation an venous fat content under in vivo conditions: a bilateral study of 13 sheep. Acta Orthop Scand 2002 Aug; 73(4):409-15